This study addressed a series of policy questions related to the impact of CHIP, the effective operation of CHIP programs, and the inter-relationship between and among CHIP, Medicaid, and employer-sponsored insurance coverage for low-income children.
The Children's Health Insurance Program Reauthorization Act of 2009 (CHIPRA) 10-State Evaluation of the Children’s Health Insurance Program (CHIP) was a congressionally mandated evaluation to explore how CHIP has evolved since its early years. This study addressed a series of policy questions related to the impact of CHIP, the design and operation of CHIP programs, and the relationship between CHIP, Medicaid, and employer-sponsored insurance coverage for low-income children. It evaluated the impacts of CHIP on children’s coverage and access to care and assessed new issues that have arisen as a result of CHIPRA and the Patient Protection and Affordable Care Act (ACA).
The Children's Health Insurance Program Reauthorization Act of 2009 (CHIPRA) 10-State Evaluation of the Children’s Health Insurance Program (CHIP) was a congressionally mandated evaluation to explore how CHIP has evolved since its early years. This study addressed a series of policy questions related to the impact of CHIP, the design and operation of CHIP programs, and the relationship between CHIP, Medicaid, and employer-sponsored insurance coverage for low-income children. It evaluated the impacts of CHIP on children’s coverage and access to care and assessed new issues that have arisen as a result of CHIPRA and the Patient Protection and Affordable Care Act (ACA).
Evaluation results are contributing to CHIP-related policy decisions, providing evidence to help policymakers decide how CHIP will be integrated into the health care system engendered by the passage of the ACA.
Mathematica’s evaluation drew on new primary data collection efforts, including surveys with parents of CHIP enrollees and disenrollees in 10 states and parents of Medicaid enrollees and disenrollees in 3 states, case studies that included focus groups with parents and interviews with key informants and stakeholders in 10 states, and a survey of program administrators in all 50 states. The evaluation also utilized secondary data sources, including the Current Population Survey, the American Community Survey, and state administrative enrollment files, to analyze participation, enrollment, and retention outcomes.
Findings
Key findings from the evaluation include the following:
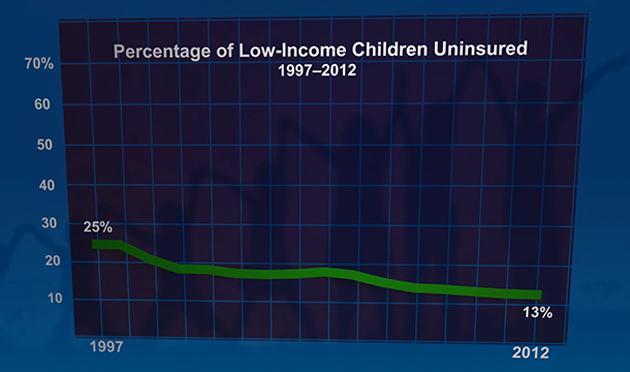
- CHIP contributed greatly to the decline in uninsured rates among low-income children, which fell from 25 percent in 1997 to 13 percent in 2012. Since CHIP was enacted, coverage rates improved for all ethnic and income groups, and coverage disparities narrowed significantly for Hispanic children.
- Nationwide, Medicaid and CHIP participation rates increased from 82 percent in 2008 to 88 percent in 2012, even as the number of eligible children has grown. The number of children eligible for Medicaid or CHIP, that remain uninsured, fell from 4.9 million in 2008 to 3.7 million in 2012.
- Relatively few low-income children in CHIP have access to private insurance coverage; the rate of children directly switching from private to public coverage at the time of CHIP enrollment was as low as 4 percent. Even when dependent coverage is available to families with children in CHIP, affordability is likely a barrier many parents face in obtaining employer-sponsored coverage for their children.
- Enrollment in both Medicaid and CHIP worked as intended to provide a safety net for low-income children, especially during economic downturns.
- Most new CHIP enrollees stayed enrolled for at least 28 months, and the vast majority left because they were no longer eligible.
- Children in Medicaid and CHIP had better access to care, fewer unmet needs, and greater financial protection than uninsured children.
- Most low-income families knew about Medicaid and CHIP, and those with children enrolled in the programs reported positive application experiences. However, some barriers to enrollment remain for eligible but uninsured children.